Choi: Effects of an EMR Education Program on Nursing Information Literacy, Self-Directed Learning, Problem-Solving Ability, and Practice Satisfaction of Undergraduate Nursing Students
Abstract
Purpose
This study implemented an electronic medical record (EMR) training program for nursing students and aimed to confirm its effectiveness.
Methods
A non-equivalent control group pretest-posttest design was used. The participants were 42 sophomore nursing students enrolled in a fundamental nursing course (experimental group: n=21, control group n=21). The EMR training program consisted of 6 sessions, taught over 5 weeks. Data were collected between April 23 and July 14, 2023, and were analyzed using the x2 test, Fisher exact test, t-test, paired t-test, Wilcoxon signed-rank test, and Mann-Whitney U test with SPSS for Windows version 24.0.
Results
Significant differences were shown between the experimental and control groups regarding self-directed learning ability (t=2.22, p=.032), problem-solving ability (t=2.34, p=.026), practice satisfaction (U=136.00, p=.016) and EMR competency (U=101.50, p=.001).
Conclusion
The EMR training program effectively improved nursing students’ self-directed learning ability, problem-solving ability, practice satisfaction, and EMR competency. Therefore, developing and applying EMR-related content can enhance nursing student's awareness of EMR systems is recommended.
Key words: Electronic health records, Nursing education, Nursing informatics, Problem-solving, Students nursing
INTRODUCTION
1. Necessity of Research
Electronic medical records (EMRs) are an essential component of digitally connected modern healthcare, and they are a secure, integrated, digital healthcare technology that embeds patient information into the healthcare systems. As of 2020, the EMR penetration rate of general hospitals in Korea is 96%, so the ability of medical personnel to use EMR is essential [ 1]. Parthasarathy et al. [ 2] reported that nurses' ability to use EMRs productively is critical to reducing healthcare costs, improving patient safety and quality of care, and facilitating efficient workflows. Under-graduate-level education in nursing schools is needed to support nurses' acquisition of nursing information competencies in a digital health environment and to strengthen their preparation for the future [ 3]. Therefore, nursing schools should provide nursing students with theoretical and technical knowledge related to these health information systems [ 4]. This is especially important given the growing concern that new nurses are unprepared to use health information systems [ 5, 6]. In nursing schools, it should begin teaching the utilization of EMR before beginning clinical practice to prepare students to navigate electronic medical records [ 7]. However, in Korea, EMR education is mainly conducted by nurses during clinical practice. EMR in hospitals is difficult to access due to the Personal Information Protection Act and the Medical Act, and it is a restrictive system that can only be used at a fixed time and place during clinical practice [ 8]. In addition, due to the busy and complex clinical environment, observation-based practice still makes it difficult for nurses to teach EMR to nursing students [ 9]. This means that EMR education takes into account the learner's situation, and students cannot practice EMR operation sufficiently, resulting in decreased satisfaction with the practice [ 5, 10]. As the need for EMR training grows, academic EMR programs are being developed. Academic EMR is defined as ‘a fully functional system that allows students to explore technology, record documentation, and plan patient care in a simulation format’ [ 11]. Academic EMR has been proposed as an innovative teaching method that facilitates the acquisition of theoretical knowledge and skills in informatics while using EMR in a familiar environment before meeting actual patients, thereby better preparing them for clinical work after graduation [ 10, 12– 14]. However, due to the high economic cost incurred when installing the academic EMR system, it has not been widely distributed to schools, so there is still a lack of reports on the effectiveness of using it. To adapt nursing students to the medical information system due to the rapid growth of medical information technology, many nursing educational institutions are adopting ‘informatics’ into their nursing curriculum [ 15]. Nursing information literacy refers to nurses' ability to recognize patients' needs, find necessary information, and effectively use it in nursing care [ 13, 14]. Prior studies have shown that nurses' lack of information literacy reduces clinical outcomes and makes it difficult to discover and use evidence [ 14, 16]. Therefore, strategies are needed to improve nursing information literacy among nursing students. EMR training is a strategy that helps improve nursing students' critical thinking and ability to navigate EMR and understand informatics concepts such as data management [ 12]. Therefore, nursing schools should support nursing students to acquire nursing information literacy competencies through EMR education [ 5]. Nursing students are required to perform electronic nursing records in various clinical settings after graduation, so they need the self-directed ability to collect, evaluate, and utilize information necessary for problem-solving or decision-making [ 13, 17]. EMR education allows users to find information within the system, such as a patient's labs and vital signs, and reflect them to enable self- care planning [ 18]. EMR training has been shown to increase students' self-directed learning capabilities compared to paper medical records [ 17, 19], but there are not many studies on this. Nurses with a high level of problem-solving skills can better use the nursing process to provide more care to their subjects [ 15]. Since the nursing part of most EMR systems is described as a procedure in the ‘nursing process’, which is a problem-solving system [ 20], it is necessary to confirm the relationship between EMR education and problem-solving skills through research on the effectiveness of EMR education. Recently, a free academic EMR platform developed by a Korean company has made EMR training possible without financial burden. Regarding academic EMR, many studies have been published on the effectiveness of EMR education in other countries [ 2, 5, 7, 10, 11, 12], but there are not many of them, such as a pilot study on the effectiveness of simulation incorporating EMR for nursing students and an evaluation of the satisfaction of electronic nursing records in Korea [ 10, 20]. Accordingly, the researchers evaluated nursing information literacy, self-directed learning, problem-solving ability, and practical satisfaction and trust in electronic records after applying the nursing record program using the free version of SMART NURSING ENR® from DK Info, an academic EMR platform provider, after self-teaching in an open lab for basic nursing for nursing students.
2. Research Purpose
This study aims to investigate the effects on nursing information literacy, self-directed learning, nursing problem-solving ability, practice satisfaction, and confidence in electronic records after applying an educational program using a simulated SMART NURSING ENR® developed for nursing students in autonomous practice.
3. Research Hypothesis
Hypothesis 1. The experimental group that participates in the EMR training program will have a higher nursing information literacy score after the completion of the program than the control group that does not participate in the program. Hypothesis 2. The experimental group that participates in the EMR training program will have a higher self-directed learning score after the completion of the program than the control group that does not participate in the program. Hypothesis 3. The experimental group that participates in the EMR training program will have a higher problem-solving ability score after the completion of the program than the control group that does not participate in the program. Hypothesis 4. The experimental group that participates in the EMR training program will have a higher nursing skill lab-practice satisfaction score after the completion of the program than the control group that does not participate in the program. Hypothesis 5. The experimental group that participates in the EMR training program will have a higher EMR confidence score after the completion of the program than the control group that does not participate in the program.
METHODS
1. Study Design
This is a quasi-experimental study to develop and apply the program based on EMR for education to investigate the effects on nursing information literacy, self-directed learning, nursing problem-solving ability, practice satisfaction, and confidence in electronic records, with non-equivalent control group pre-and post-study design ( Figure 1).
Figure 1.
Flowchart of the research design and process. 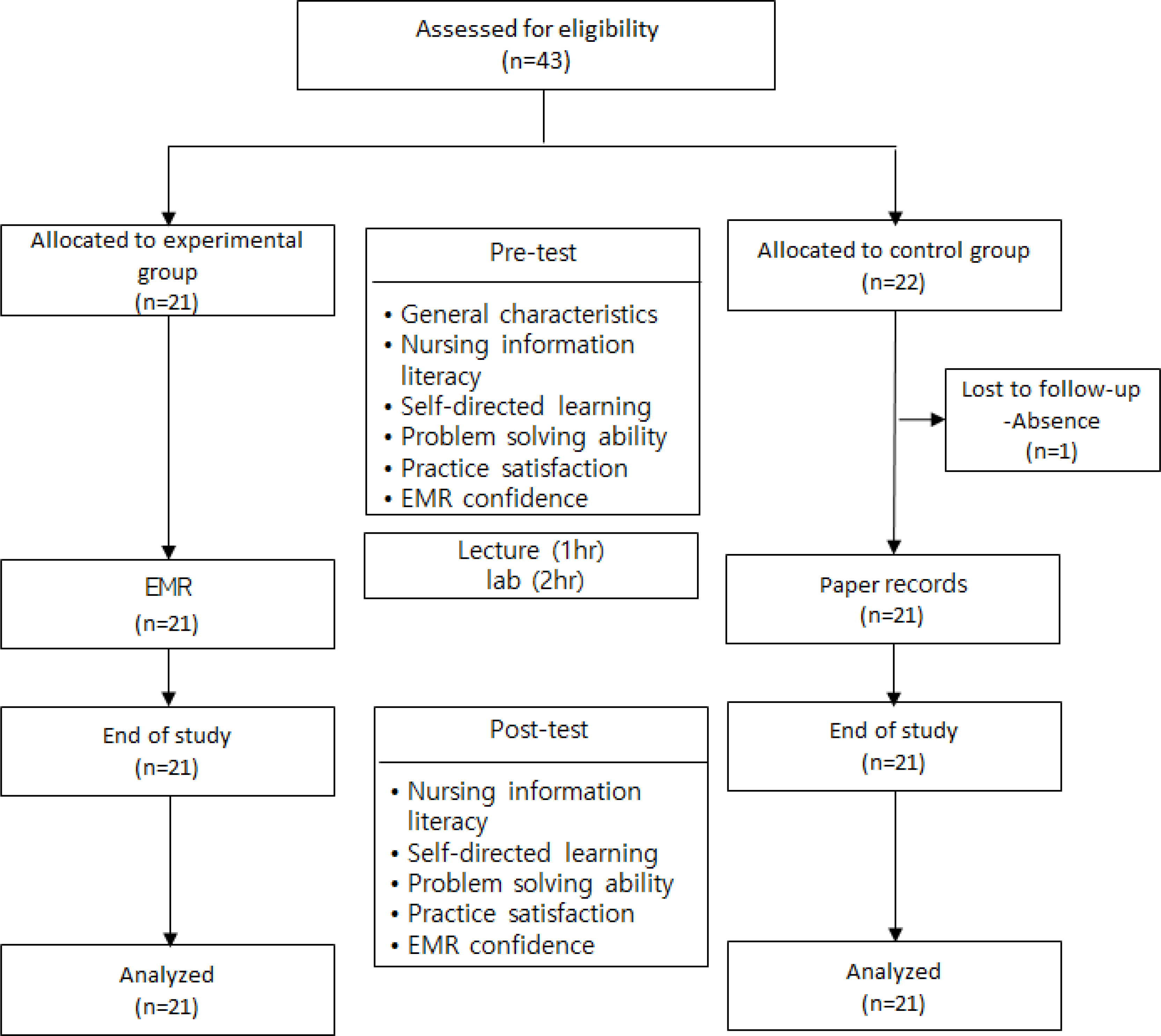
2. Study Participants
The participants of this study were second-year nursing students enrolled in a university located in I City, who understood the purpose of this study and agreed to participate. Participants were divided into two groups and then randomly assigned to the experimental and control groups by drawing lots. The detailed inclusion criteria were 1) second-year nursing students taking fundamental nursing and practicum courses and 2) those who have studied the ‘Nursing Records’ chapter of fundamental nursing and have a theoretical understanding of nursing records. Those who withdrew their participation in the study due to a leave of absence were excluded.
The G*Power 3.1.9.2 program was used to calculate the number of samples. Based on a previous study [ 21] in which a one-sided test was selected to confirm a significant difference in a small group of subjects, the minimum number of samples required per group was 18, considering the significance level of .05, power of 80%, and effect size of 0.85 in the mean comparison of the two independent sample groups. Considering the dropout rate (15%), the subjects recruited were 21 in the experimental group, and 22 in the control group, and 1 person who took a leave of absence from school in the experimental group was eliminated, so the final subjects were 21 in each group, for a total of 42( Figure 1).
3. Data Collection and Research Procedure
In this study, data were collected during the open-lab practice of fundamental nursing from April to July 2023. Fundamental nursing classes to learn the basic knowledge of vital signs, drainage tube management, simple catheterization, and indwelling catheterization, and fundamental nursing practice classes and self-practice classes that show the performance process of each skill were the same for both the experimental and control groups. Among the core skills in fundamental nursing practice contents, vital sign measurement, drainage tube management, simple catheterization, and indwelling catheterization were selected, and the protocol of these skill items includes clinical observation records and nursing records, which are important in clinical nursing. The specific research procedure is as follows.
1) EMR program for learning
EMR for learning used SMART NURSING ENR ®, a free training program developed by DKMediInfo. SMART NURSING ENR ® is a cloud-based EMR learning system developed to fill out various record forms online. In this study, with the permission of the developer, it was used as a basis for the cases developed for nursing records after practicing vital signs, drainage tube management, simple catheterization, and indwelling catheterization. Three fundamental nursing professors reviewed each case for adequacy to ensure that it was appropriate for the 2nd year level. As a result of the review, it was suggested to mirror a sample of records in the first EMR training and to have a general reflection time in the last session ( Table 1).
Table 1.
EMR Training program for Undergraduate Nursing Students
|
Session |
Component |
Contents |
Method |
Time (min) |
|
1 |
Pre-lecture on EMRs |
․ A general description of nursing records |
Lecture |
60 |
|
․ Concept, necessity, and type of nursing records (SOAPIE, DAR, narrative record), nursing process, recording methods (based on paper) Definition and necessity of EMR; providing nursing record screen actually used in hospitals |
|
2 |
Orientation |
․ Introduction to the EMR training program; organizing and naming small groups; introducing the group moderator and group members |
Lecture practice |
30 |
|
․ How to access the EMR program; signing up for the EMR program through a personal laptop or tablet PC, logging in, and opening the record form for each item provided on the EMR screen and explaining how to enter it |
|
․ Explanation of practice-related situational cases (inpatients, postoperative drainage tube management, insertion of catheterization to measure excretion, and management of dysuria) provided with each practice (vital signs, drainage tube management, simple and catheterization) |
|
3 |
EMR training 1 |
․ Educational module: EMR through inpatient care cases |
Open lab self-practice |
60 |
|
․ Provide a demonstration of how to use the EMR |
EMR practice |
30 |
|
․ Input nursing records on the EMR screen; clinical observation records, inpatient nursing record |
|
4 |
EMR training 2 |
․ Educational module: Postoperative drainage tube management |
Open lab self-practice |
60 |
|
․ Feedback on previous records: After entering the nursing record, the instructor provides online feedback on the student's record; the feedback is accompanied by supplementary data on deficiencies in nursing records |
EMR practice |
30 |
|
․ Nursing records, such as vital signs records, prescription confirmations, clinical observation records, and the use of pain assessment tools, are prepared according to practice-related situational cases |
|
5 |
EMR training 3 |
․ Educational module: Insertion of an indwelling catheter to measure excretion |
Open lab self-practice |
60 |
|
․ Feedback on previous records |
EMR practice |
30 |
|
․ Nursing records, including clinical observation records, I/O, and SOAPIE according to practice-related cases |
|
6 |
EMR training 4 |
․ Education module: management of dysuria |
Open lab self-practice |
60 |
|
․ Feedback on previous records |
EMR practice |
50 |
|
․ Nursing records include vital signs, clinical pathology, verbal prescription, clinical observation, I/O, post-intervention evaluation, and narrative records according to practice-related situation cases |
|
․ Overall evaluation of the program |
2) Pre-test
Before treatment, the general characteristics of the subjects, nursing information literacy, self-directed learning, nursing problem-solving ability, practice satisfaction, and confidence in electronic records were measured by surveying with an online questionnaire program (Google Drive, Naver Questionnaire).
3) Pre-education
Both the experimental and control groups were educated on the basic types of records, recording methods (on paper), and nursing procedures and nursing records (Subjective data, Objective data, Access, Plan, Implementation, Evaluation, SOAPIE; Data, Action, Response, DAR) during the ‘ recording and reporting’ unit classes. Practice-related situational cases (inpatient-vital sign, postoperative drainage tube management- drainage tube management, indwelling catheter insertion to measure excretion-indwelling catheter insertion, management of patients with dysuria-simple catheter insertion) were also described along with each practice.
4) Experimental group treatment
The EMR education program provided to the experimental group was conducted in 6 rounds, excluding pre- training, and was conducted once a week. At the orientation, training was provided on how to access the SMART NURSING ENR® used in this study and how to enter clinical observation records and nursing records (SOAPIE, DAR) on the EMR program. After the self-practice in the open lab for 1 hour performed according to the inpatient nursing case used in the first vital sign practice, the EMR program was opened, and the clinical observation record, SOAPIE and narrative record were shown, and the students were asked to enter the vital sign measurement and nursing record as shown using each individual's laptop or tablet. From the second drainage tube management exercise, each practice-related situation includes a different form from the previous round. They were asked to fill out their nursing records, and the entire record entry was usually performed for 30~110 minutes per session. After recording, the instructor provided online feedback on what the student had recorded. In each feedback, supplementary points were made for deficiencies in nursing records. In the sixth round, after entering the nursing records for a given case, the overall evaluation of the entire program was shared with the students. In the EMR practice according to each scenario, the researcher directly guided the system access, recording, and evaluation as an instructor.
5) Control group treatment
The control group was also given a written record form for practice for 30~50 minutes per session, and how to fill it out was educated. In the case of the control group, there was no need to check the clinical test results or previous records included in the EMR, so the treatment time was shorter than that of the experimental group. After the self-practice in an open lab of 1 hour carried out with the case, the nursing records for the same situation case were written on a record sheet. If there were any flaws in the recording, the instructor would immediately pick up any minor errors on the spot, review the submission sheet, and provide feedback in the next session if necessary.
6) Post-test
A week after the end of the program, nursing information literacy, self-directed learning, nursing problem-solving ability, practice satisfaction, and confidence in electronic records were measured by surveying online questionnaire programs (Google Drive, Naver Survey).
4. Measurement
1) Nursing information literacy
The nursing information literacy competency for nurse measurement tool developed by Jo and Ha [ 14] was modified by Jo and Gu [ 13] to suit nursing students with no clinical practice experience. The contents of the tool consist of 7 domains, including 4 questions on problem identification, 5 questions on identifying information sources, 3 questions on information search, 5 questions on information evaluation, 4 questions on information acquisition and management, 2 questions on information integration, and 2 questions on information ethics, for a total of 25 questions. Each item is measured on a 5-point Likert scale, ranging from 1 for ‘not at all’ to 5 for ‘very much,’ and a higher score indicates higher nursing information literacy. The reliability of the instrument was .93 in Cronbach's ⍺ in the study of Jo and Ha [ 14], .96 in the modified study [ 13], and .96 in this study.
2) Self-directed learning
The Self-Directed Learning Ability Inventory developed by Bae and Lee [ 16] was used. This tool consists of 3 questions on learning process management and 3 questions on learning result evaluation corresponding to the cognitive domain, 3 questions on learning motivation and 3 questions on self-concept corresponding to the defining domain, 3 questions on the persistence of learning activities corresponding to the behavioral domain, 3 questions on the use/management of learning resources, and 3 questions on the creation of a learning environment. Each item is measured on a 5-point Likert scale, ranging from 1 ‘not at all’ to 5 ‘very much’, and a higher score indicates a higher self-directed learning ability. The reliability of the tool was .79 in Cronbach's ⍺ in the study of Bae and Lee [ 16] and .98 in this study.
3) Problem-solving skills
The Korean ‘ Problem solving process inventory’ developed by Lee et al. [ 22] was used. The tool consists of 5 domains: 6 questions for clarifying the problem, 6 questions for finding a solution, 6 questions for decision-making, 6 questions for implementing solutions, and 6 questions for evaluation and reflection, for a total of 30 questions. Each item is measured on a 5-point Likert scale, ranging from 1 ‘very rarely’ to 5 ‘very often’, with higher scores indicating higher problem-solving skills. The reliability of the tool was .93 in Cronbach's ⍺ in Lee et al.'s study [ 22] and .96 in this study.
4) practice satisfaction
Practice satisfaction was based on the learning satisfaction evaluation tool developed by Yoo [ 23], and the practice satisfaction tool modified and supplemented by Chang and Park [ 24] was used after the content validity of three nursing professors. This tool consists of a total of 17 questions, and each item was measured on a 5-point Likert scale from 1 point of ‘not at all’ to 5 points of ‘definitely so’, and the score range was 17~85 points, with a higher score indicating higher satisfaction with autonomous practice. The reliability Cronbach's ⍺ was .94 in Yoo's study [ 23], .89 in the modified study [ 24], and .96 in this study.
5) Confidence in electronic records
Confidence in electronic records is a measure of confidence in performing nursing records in electronic medical records, and was measured by numeric rating scale (NRS). The score was scored from a minimum of 0 (not at all confident) to a maximum of 10 (very confident) by asking the subjects to select a point on a continuous line. The higher the score, the higher the EMR confidence.
5. Data Analysis
The collected data were analyzed according to the purpose of the study using SPSS 24.0 Program.
General characteristics of the subjects were analyzed with frequency, percentage, mean, and standard deviation The normality test for the study variables was performed using the Shapiro-Wilk test. To verify the homogeneity of characteristics and study variables between the experimental and control groups, x2 test, Fisher's exact test, and t-test were used. The differences in nursing information literacy, learning self-direction, problem-solving ability, and critical thinking ability between the experimental and control groups after experimental treatment were analyzed by independent t-test and paired t-test as they approximated the normal distribution of the Shapiro- Wilk test results, and the difference in practice satisfaction did not show a normal distribution, so it was analyzed by Wilcoxon signed-rank test and Mann Whitney U test.
6. Ethical Considerations
This study was conducted upon review and approval (IRB No. 2023-ICCU-IRB-03) of Institutional Review Board in I University before the test. In this study, EMR training was conducted separately during open nursing skill-lab time outside of class hours. The researcher distributed the URL of the online questionnaire to students who wished to participate in the study, and provided the study description and consent form online. After carefully reading and understanding the purpose, process and the duration of the study, no disadvantages such as grades due to non- participation in the study, confidentiality and anonymity, they were asked to fill out an online questionnaire after filling in the name and date that would appear only if they wished to participate if they checked the word ‘I agree’ in the same sense as their signature. Subjects completed the online questionnaire in an instructor-free space where they could go online without instructor influence and had privacy, and that the data would not be used for any purpose other than research. Subjects who participated in the study were provided with small rewards, and the control group was provided with EMR training on the SMART NURSING ENR® access method, clinical observation record, and nursing record method applied to the experimental group after the follow-up investigation, and provided a learning opportunity to record online.
RESULTS
1. Homogeneity Test
As a result of testing the homogeneity of the general characteristics of the experimental and control groups of the study subjects, there was no statistically significant difference in age, gender, religion, academic performance in the previous semester, satisfaction with school life, and satisfaction with majors, so the two groups were homo-geneous. As a result of testing the homogeneity of the pre- dependent variables of the two groups, there was no statistically significant difference in nursing information literacy, learning self-direction, problem-solving ability, and practice satisfaction, so the two groups were homoge-neous ( Table 2).
Table 2.
Homogeneity Test for General Characteristics and Dependent Variables between Experimental and Control Groups (N=42)
|
Variables |
Categories |
Exp. (n=21) |
Cont. (n=21) |
x2 or t or U |
p
|
|
n (%) or M± SD |
n (%) or M± SD |
|
Age (year) |
|
22.24±6.27 |
20.05±1.36 |
1.57 |
.132 |
|
Gender |
Male |
2 (9.5) |
5 (23.8) |
1.54 |
.410†
|
|
Female |
19 (90.5) |
16 (76.2) |
|
|
|
Satisfaction with the major |
|
3.90±0.63 |
3.67±0.73 |
1.14 |
.263 |
|
Grade point average |
<3.5 |
4 (19.0) |
11 (52.4) |
5.08 |
.052†
|
|
≥3.5 |
17 (81.0) |
10 (47.6) |
|
|
|
Necessity of EMR education |
|
3.95±0.50 |
4.10±0.70 |
-0.78 |
.179‡
|
|
Necessity of information literacy education |
|
3.67±0.80 |
3.57±0.93 |
-0.01 |
.500‡
|
|
Nursing information literacy |
|
3.56±0.57 |
3.46±0.54 |
1.24 |
.546 |
|
Self-directed learning ability |
|
3.78±0.58 |
3.78±0.53 |
-0.03 |
.979 |
|
Problem-solving ability |
|
3.86±0.35 |
3.69±0.51 |
1.24 |
.221 |
|
Practice satisfaction |
|
4.11±0.46 |
3.99±0.41 |
168.50 |
.389‡
|
|
EMR Competency |
|
4.38±1.94 |
4.52±1.63 |
220.50 |
.503‡
|
2. Hypothesis Test
1) First hypothesis
The mean of nursing information literacy in the experimental group increased significantly after the test compared to the pre-test (t=-2.49, p=.022), but there was no significant difference between pre- and post-scores between the two groups (t=0.74, p=.466). Therefore, hypothesis 1 that ‘ Experimental group that participate in EMR training program will have higher nursing information literacy score after the completion of the program than the control group that does not participate in the program’ was rejected ( Table 3).
Table 3.
Comparisons of Pre-test and Post-test Results between the Experimental and Control Groups (N=42)
|
Variables |
Group |
Pre-test |
Post-test |
t or z |
p
|
Difference |
t or U |
p
|
|
M± SD |
M± SD |
M± SD |
|
Nursing information literacy |
Exp. |
3.56±0.57 |
3.86±0.32 |
-2.49 |
.022 |
0.29±0.54 |
0.74 |
.466 |
|
Cont. |
3.46±0.54 |
3.49±0.55 |
-0.37 |
.716 |
0.18±0.47 |
|
|
|
Self-directed learning ability |
Exp. |
3.78±0.58 |
3.87±0.52 |
-0.96 |
.350 |
0.09±0.42 |
2.22 |
.032 |
|
Cont. |
3.78±0.53 |
3.55±0.48 |
2.09 |
.050 |
-0.24±0.52 |
|
|
|
Problem-solving ability |
Exp. |
3.86±0.35 |
4.07±0.33 |
-3.89 |
.001 |
0.21±0.24 |
2.34 |
.026 |
|
Cont. |
3.69±0.51 |
3.63±0.49 |
0.60 |
.557 |
-0.06±0.46 |
|
|
|
Practice satisfaction |
Exp. |
4.11±0.46 |
4.50±0.40 |
-3.60 |
<.001†
|
0.39±0.36 |
136.00 |
.016‡
|
|
Cont. |
3.99±0.41 |
4.09±0.43 |
-1.92 |
.028†
|
0.10±0.40 |
|
|
|
EMR competency |
Exp. |
4.38±1.94 |
5.71±1.71 |
-2.72 |
.013 |
1.33±2.24 |
101.50 |
.001‡
|
|
Cont. |
4.52±1.63 |
4.29±1.19 |
1.05 |
.309 |
-0.24±0.04 |
|
|
2) Second hypothesis
The self-directed learning in the experimental group increased by 0.09 points from 3.78 points before to 3.87 points after the intervention, and the control group decreased by 0.24 points from 3.78 points to 3.55 points after the intervention, indicating a statistically significant difference between pre- and post-scores between the two groups (t=2.22, p=.032). Therefore, hypothesis 2 that ‘Experimental group that participate in EMR training program will have higher self-directed learning score after the completion of the program than the control group that does not participate in the program’ was accepted ( Table 3).
3) Third hypothesis
The problem-solving ability of the experimental group increased by 0.21 points from 3.86 points before to 4.07 points after the intervention on a 5-point scale, indicating a statistically significant difference (t=-3.89, p=.001), and the control group decreased by 0.06 points from 3.69 points to 3.63 points after the fact, indicating that there was a statistically significant difference between pre- and post-scores between the two groups (t=2.34, p=.026). Therefore, hypothesis 3 that ‘ Experimental group that participate in EMR training program will have higher problem-solving ability score after the completion of the program than the control group that does not participate in the program’ was accepted ( Table 3).
4) Fourth hypothesis
Practice satisfaction of the experimental group increased by 0.39 points (z=-3.60, p<.001) from 4.11 points before to 4.50 points after the test on a 5-point scale, and by 0.10 points (z=-1.92, p=.028) from 3.99 points to 4.09 points after the fact in the control group (z=-1.92, p=.028), indicating that there was a statistically significant difference between pre- and post-scores between the two groups (U=136.00, p=.016). Therefore, Hypothesis 4 that ‘ Experimental group that participate in EMR training program will have higher nursing skill lab-practice satisfaction score after the completion of the program than the control group that does not participate in the program’ was accepted ( Table 3).
5) Fifth hypothesis
EMR confidence in the experimental group increased by 1.33 points from 4.38 points before to 5.71 points after the test on a 10-point scale, showing a statistically significant difference (z=-2.72, p=.013), and the control group decreased by 0.24 points from 4.52 points before to 4.29 points after the fact, indicating a statistically significant difference between pre- and post-scores between the two groups (U=101.50, p=.001). Therefore, hypothesis 5 that ‘ Experimental group that participate in EMR training program will have higher EMR confidence score after the completion of the program than the control group that does not participate in the program’ was accepted ( Table 3).
DISCUSSION
This study presented the effect of nursing record education using the academic EMR system in the open lab time of fundamental nursing. The significance of this study is that it provided usable methodological evidence for effective EMR education in a situation where there are few studies that have identified the effectiveness of EMR education in Korea.
The Academic EMR program used in this study is a cloud-based electronic nursing record system for learning, which can be implemented in both PC and mobile applications, and in particular, it is equipped with cases in con-nection with fundamental nursing practice, so it is possible to train electronic nursing records according to practice according to the flow of the curriculum. In this study, in order to improve the abilities of second-year nursing students who have not completed nursing informatics and clinical practice, five modules consisting of topics covered in fundamental nursing were developed and applied to practice, self-practice, electronic nursing records, and feedback.
First, compared to before the experiment, the nursing information literacy of the experimental group improved significantly after the completion of the program, but there was no significant difference between the experimental group and the control group. This is different from a previous study [ 11] in which third-year nursing informatics students improved their information skills after EMR training. In the case of this study, both the experimental and control groups had high nursing information literacy scores before the experiment, and it is thought that it was difficult to show an immediate change in competence due to the short EMR training period of 4 sessions. In addition, the measurement tool used in this study consists of a query item on the comprehensive utilization of nursing information, and it is presumed that it would have been difficult to accurately grasp nursing information literacy through EMR without nursing and clinical practice experience. Therefore, an appropriate study design is needed to validate nursing literacy and to develop tools focused on the use of EMR. In this study, nursing students' self-directed learning was significantly improved in the experimental group compared to the control group. This is similar to Lin et al. [ 17]'s report that PBL-linked EMR training is effective in self-directed learning among nursing students in Taiwan and supports previous research that EHR training for medical students promotes self-directed learning [ 19]. The academic EMR system used in this study was equipped with virtual data such as clinical observation records, clinical pathology records, prescriptions, and hospitalization records so that learners could show higher concentration by selecting the necessary information through various patient information channels. In addition, due to the nature of the online system, it is believed that it would have contributed to the improvement of the subject's self-direction by promoting individual learning regardless of any place and time outside of class time. In this regard, Choi's study [ 11] found that EMR training through mobile devices such as tablet PCs and cell phones helps improve accessibility. In this study, many students typed using mobile devices, and when they did not complete the input within the program time, they switched to assignments and were encouraged to complete them on their own. This could be presented as a method of online nursing education in a pandemic such as COVID-19. The problem-solving ability of nursing students was significantly improved in the experimental group compared to the control group. There were few prior studies examining the effects of EMR training on problem-solving ability, making it difficult to make a direct comparison. Considering that EMR education can ultimately lead to improved nursing information literacy [ 11, 25], the discussion points were inferred from previous studies [ 13, 14, 26] that analyzed the relationship between nursing information literacy and problem-solving ability. A study by Jo and Gu et al.[ 13] showed that nursing information literacy had a direct effect on problem-solving ability among nursing students, while a study by Kwak et al. [ 14] and Ha et al. [ 26] showed that nursing information literacy was highly correlated with problem-solving ability. This suggests that the use of EMR in the experimental group in this study may have had an effect on the improvement of problem- solving ability. In this program, students read the nursing problem scenario in the module and performed self-practice, and then systematically recorded nursing through SOAPIE and DAR forms while recognizing the basis for the practice (prescription organized according to test result data and cases). Since this learning structure clarified the problem-solving process, it is thought that the problem-solving ability of the experimental group improved. Satisfaction with the nursing lab practice of nursing students was significantly improved in the experimental group compared to the control group. This is in a similar to the study by Kim and Kim et al. [ 27], who reported that classes using virtual reality increased educational satisfaction, given that the academic EMR system is composed of virtual data. This is supported by focus group interviews and Hong et al.[ 10] who reported that the participants in the simulation education incorporating AEMRs were sat-isfied and confident in their practice. In traditional practice, EMR has been difficult to access due to limitations such as ethical issues in the reading of patient information and interference with the work of clinical nurses. In this study, the EMR program was applied in the self-practice situation of the nursing skill open-Lab for second-year subjects with no experience in nursing informatics and clinical practice, and it was possible to increase the satisfaction of nursing students. Practical education using virtual EMR content tailored to the scenario is an attractive learning medium for nursing students because it has a sense of presence so that they can vicariously experience EMR in clinical practice. There is no concern about maladaptation to practice due to unfamiliarity with EMR in clinical practice, and it is possible to repeat learning regardless of the place depending on the platform [ 28]. These advan-tages suggest the need to expand the development and application of EMR contents that reflect actual reality not only in clinical practice but also in the training of new nurses. On the other hand, the subjects of this study are a digital generation with an average age of 21 years and use digital technology for a considerable amount of time. They fre-quently use smartphones, UCC (User Created Contents), and SNS (Social Network Service), and are accustomed to audiovisual learning methods using various communication media [ 29]. This is supported by a study by Jung et al. [ 30], which pointed out that immaturity in the technology to utilize online media affects educational satisfaction. In addition, the experiment group showed a higher level of satisfaction with the practice because the students had the opportunity to review their practice process through the instructor's feedback on EMR and decide on what behaviors should be supplemented to obtain better results. Unusually, the control group also reported higher satisfaction with the practice after the treatment than before. This reflects the characteristics of open-lab practice for lower grades, which means that additional learning opportunities such as clinical recording training and feedback along with non-proficient practice can increase practice satisfaction [ 31]. In the future, methodological research and its application to improve the quality of open-lab practice need to be expanded. The experimental group showed a significant improvement in student's EMR confidence compared to the control group after the experiment. This is consistent with the findings of a previous study [ 32] that reported the effect of applying EMR training on increased self-confidence. Ruckdeschel [ 33] reported that EMR was not addressed in schooling, and nursing students or new nurses reported initial anxiety about EMR in hospitals. In this study, it is thought that the confidence of electronic records was increased by increasing access to EMR programs and systematically entering situations after scenario-based exercises rather than one-time training. On the other hand, previous studies applying EMR to simulation practice have reported that EMR helps students improve their ability to process electronic documents [ 27] and develop pos-itive attitudes and perceptions of electronic records [ 16, 32]. The integrated application of EMR in simulation classes improves students' confidence and self-efficacy in the use of electronic records [ 5, 12] and improves their informatics knowledge and abilities [ 10, 11]. These benefits are why efforts to extend EMR to nursing education should continue. In addition, in this study, it was for second-year students in the basic stage, but in the case of older students, it is expected that EMR confidence will be higher if it is linked to simulation practice, so it is proposed to develop scenarios based on more delicate and diverse situations for older students in the future and study them in conjunction with simulation practice. Based on the results, it was found that using academic EMR programs are very effective in improving nursing students' self-directed learning, problem-solving ability, practice satisfaction, and EMR confidence. Therefore, it is necessary to develop and apply various EMR contents that can enhance the sense of reality of EMR among nursing students.
The limitations of this study are that it is difficult to generalize the conclusions due to the lack of representation and small sample size of the convenience sample of sec-ond-year nursing students at a university, and it may be difficult to establish internal validity of the study because it was difficult to form an independent situation with the research participants because the researcher who is a professor led the program. Based on the above results, the following suggestions were derived. First, more nursing schools need to expand the number of subjects in the study to revalidate the results. Second, there is a need for further research to develop EMR content on various nursing topics for older nursing students and evaluate their effectiveness after using it. Third, to reduce the threat of internal validity due to bias in the relationship between researcher and subject in future similar studies, it is necessary for a trained third party, not the researcher, to be in charge of training and measurement.
CONCLUSION
This study found that academic EMR programs are effective in improving self-directed learning, problem-solving skills, practice satisfaction, and EMR confidence. The significance of this study lies in the fact that the effect of the EMR education program was confirmed by applying the nursing problem situation module created for the EMR program to second-year nursing students. Based on this study, it is expected that the development and application of various EMR contents that can enhance the sense of reality of EMR among nursing students will be expanded.
REFERENCES
1. Lee JH. Report on the survey of health and medical Information in 2020. Seoul: Ministry of health and welfare; Korea health information service; 2021 April. p. 4.
3. Technology Informatics Guiding Education Reform. The TIGER initiative, information competencies for every practicing nurse: Recommendations from the TIGER collaborative [Internet]. Chicago: Technology Informatics Guiding Education Reform; 2009. [cited 2023 September 29]. Available from: https://tigercompetencies.pbworks.com/f/TICC_Final.pdf
4. Nagle LM, Kleib M, Furlong K. Digital health in Canadian schools of nursing part A: nurse educators' perspectives. Qual-ity Advancement in Nursing Education-Avancees en Formation Infirmiere. 2020; 6(1):1-19. https://doi.org/10.17483/2368-6669.1229
 6. Shin EH, Cummings E, Ford K. A qualitative study of new graduates' readiness to use nursing informatics in acute care settings: clinical nurse educators' perspectives. Contemporary Nurse. 2018; 54(1):64-76. https://doi.org/10.1080/10376178.2017.1393317
 7. George NM, Drahnak DM, Schroeder DL, Katrancha ED. Enhancing prelicensure nursing students' use of an electronic health record. Clinical Simul in Nursing. 2016; 12(5):152-158. https://doi.org/10.1016/j.ecns.2015.11.006
8. Korea ministry of government legislation. Introduction of Korean law information [Internet]. Sejong-si: Korea ministry of government legislation; 2024. [cited 2024 January 1]. Available from: https://www.law.go.kr
11. Choi M, Park JH, Lee HS. Assessment of the need to integrate academic electronic medical records into the undergraduate clinical practicum: a focus group interview. Computers Informatics Nursing. 2016; 34(6):259-265. https://doi.org/10.1097/CIN.0000000000000244
12. Mollart L, Newell R, Geale SK, Noble D, Norton C, O'Brien AP. Introduction of patient electronic medical records (EMR) into undergraduate nursing education: an integrated literature review. Nurse Education Today. 2020; 94: 104517. https://doi.org/10.1016/j.nedt.2020.104517
13. Jo MJ, Gu MO. Development and effects of a nursing information literacy competency education program for undergraduate nursing students. Journal of Korean Academy Society of Nursing Education. 2021; 27(2):210-222. https://doi.org/10.5977/jkasne.2021.27.2.210
14. Kwak SO, Kim YS, Lee KJ, Kim M. Influence of nursing informatics competencies and problem-solving ability on nursing performance ability among clinical nurses. The Journal of Korean Academic Society of Nursing Education. 2017; 23(2):146-155. https://doi.org/10.5977/jkasne.2017.23.2.146
15. Kim SE, Lee MH. An exploratory study on the effectiveness of information literacy education for college students. Journal of Korean Library and Information Science Society. 2007; 38(3):91-115. https://doi.org/10.5977/jkasne.2016.22.3.396
16. Foster M, Sethares K. Current strategies to implement informatics into the nursing curriculum: An integrative review. On-Line Journal of Nursing Informatics. 2017; 21(3):1-4.
17. Bae EK, Lee MY. The development of the self-directed learning ability inventory for employees in HRD companies. The Korean Journal of Human Resource Development. 2010; 12(3):1-26. 18. Lin CL. Applying self-directed learning with virtual electronic medical records learning system for nursing students. Poster session presented at: 33rd. International research congression. 2022 July 21-25. Edinburgh, Scotland..
20. Stayt LC, Merriman C, Ricketts B, Morton S, Simpson T. Recognizing and managing a deteriorating patient: a randomized controlled trial investigating the effectiveness of clinical simulation in improving clinical performance in undergraduate nursing students. Journal of Advanced Nursing. 2015; 71(11):2563-2574. https://doi.org/10.1111/jan.12722
21. Kim SE, Lee MH. An exploratory study on the effectiveness of information literacy education for college students. Journal of Korean Library and Information Science Society. 2007; 38(3):91-115. https://doi.org/10.5977/jkasne.2016.22.3.396
22. Ryoo EN, Ha EH, Cho JY. Comparison of learning effects using high fidelity and multimode simulation: an application of emergency care for a patient with cardiac arrest. Journal of Korean Academy of Nursing. 2013; 43(2):185-193. https://doi.org/10.4040/jkan.2013.43.2.185
23. Lee WS, Park SH, Choi EY. Development of a Korean problem-solving process inventory for adults. Journal of Korean Academy of Fundamentals of Nursing. 2008; 15(4):548-557.
24. Yoo MS. The effectiveness of standardized patient managed instruction for a fundamental nursing course. Journal of Korean Academic Society of Nursing Education. 2001; 7(1):94-112.
25. Whitt KJ, Eden L, Merrill KC, Hughes M. Nursing student experiences regarding safe use of electronic health records: a pilot study of the safety and assurance factors for EHR resil-ience guides. Computer Informatic Nursing. 2017; 35(1):45-53. https://doi.org/10.1097/CIN.0000000000000291
26. Ha YM, Lee M, Chae YJ. The effectiveness of nursing information literacy competency enhancement program on evi-dence-based practice competencies and problem-solving skills in nursing students. Journal of Digital Convergence. 2016; 14(11):347-356. https://doi.org/10.14400/JDC.2016.14.11.347
27. Kim MG, Kim HW. The effects of classes using virtual reality simulations of the hospital environment on knowledge of the hospital environment, academic self-efficacy, learning flow, educational satisfaction and academic achievement in nursing students. Journal of Korean Academy of Fundamental Nursing. 2021; 28(4):520-529. https://doi.org/10.7739/jkafn.2021.28.4.520
29. Song SR, Kim YJ. Effect of a self-evaluation method using video recording on competency in nursing skills, self-directed learning ability, and academic self-efficacy. Journal of Korean Academy of Fundamentals of Nursing. 2015; 22(4):416-423. https://doi.org/10.7739/jkafn.2015.22.4.416
30. Jung EY, Park DK, Lee YH, Jo HS, Lim YS, Park RW. Evaluation of practical exercises using an intravenous simulator incorporating virtual reality and haptics device technologies. Nurse Education Today. 2012; 32(4):458-463. https://doi.org/10.1016/j.nedt.2011.05.012
31. Chang E, Park S. Effects of self-evaluation using smartphone recording on nursing students' competency in nursing skills, satisfaction, and learning motivations: Focusing on foley catheterization. Journal of Korean Academy of Fundamentals of Nursing 2017; 24(2):118-127. 32. Mollart L, Newell R, Noble D, Geale S, Norton C, O'Brien A. Nursing undergraduates' perception of preparedness using patient electronic medical records in clinical practice. Austral-ian Journal of Advanced Nursing. 2021; 38(2):44-51. https://www.ajan.com.au/index.php/AJAN/article/view/282
33. Ruckdeschel AR. Electronic health record instruction in first- semester nursing students: A comparative study [dissertation]. Las Vegas: University of Nevada; 2018. p. 7-8.
|
|











