








INTRODUCTION
Mechanical ventilation should be applied to patients with respiratory failure who are unable to breathe sponta-neously and exchange gas. The function of the mechanical ventilator is to maintain gas exchange and meet the patient's metabolic requirements by regulating pressure or tidal volume [1]. Therefore, nurses must have specialized knowledge and skills related to mechanical ventilator management in order to care for severely ill patients with respiratory failure, and should be well trained from the time they are students. Before practicing in the intensive care unit, nursing students must be trained in advance knowledge and skills on unfamiliar machines such as ven-tilators to gain a positive practice experience [2]. Essential knowledge for mechanical ventilation includes respira-tory system anatomy, physiology, artery blood gas analy-sis (ABGA), ventilator settings, mode types, complication prevention, and alarm sound response. Its content is broad and professional [3]. Nurse's skills, such as connecting circuits correctly, ensuring the appropriate mode for the patient, and responding to alarms immediately, are crit-ical to keeping patients safe. Thus, this ability can prevent problems such as airway aspiration and ventilator-related pneumonia [4]. In previous studies related to mechanical ventilation education, information on infection manage-ment related to ventilators was available for students and clinical nurses, as well as web-based learning and simu-lations for students [5–13]. However, there were limitations in improving performance ability through online learning. Also the simulation practice did not have enough time for pre-learning.
Blended learning is an education method that combines the advantages of online and offline instruction. The ad-vantage of face-to-face education is realistic interaction, and the advantages of online education are that group class time is minimized and prior learning or review is possible without time and space constraints [14]. For stu-dents who are proficient in information technology, the combination of online education using the university's learning management system (LMS) and practice education is an effective teaching method. Mechanical ventilation education should not only convey knowledge but also provide opportunities for hands-on practice. To raise the cognitive domain of educational goals to a higher level of application, analysis, and evaluation, mechanical ventilation instruction should be given using as a learning meth-od with which learners can talk, think, and perform a lot [15]. However, blended learning, which is a combination of online and face-to-face learning, is suitable for learning complex and specialized knowledge and skills such as ventilator management, but research on such blended learning related to mechanical ventilation is absent. It is necessary to develop effective teaching methods for nursing students who do not have experience or training in ventilator management [16]. Therefore, this study would develop a mechanical ventilation education program with blended learning that enables nursing students to system-atically acquire knowledge and nursing skills according to their needs. The program developed in this study could be used for practice in critical care nursing. An improvement in students' confidence will also result. The hypotheses of this study are as follows.
• Hypothesis 1. The experimental group with blended learning will have a higher level of knowledge of me-chanical ventilation than the control group with on-line education only.
• Hypothesis 2. The experimental group with blended learning will have higher self-confidence level than the control group with online education only.
• Hypothesis 3. The experimental group with blended learning will have a higher level of ventilator nursing skills performance than the control group with online education only.
METHODS
1. Study Design
This study was a quasi-experimental design and non-equivalent comparison group before and after design to verify the effect of a ventilator-education program using a blended learning method for nursing students.
2. Participants
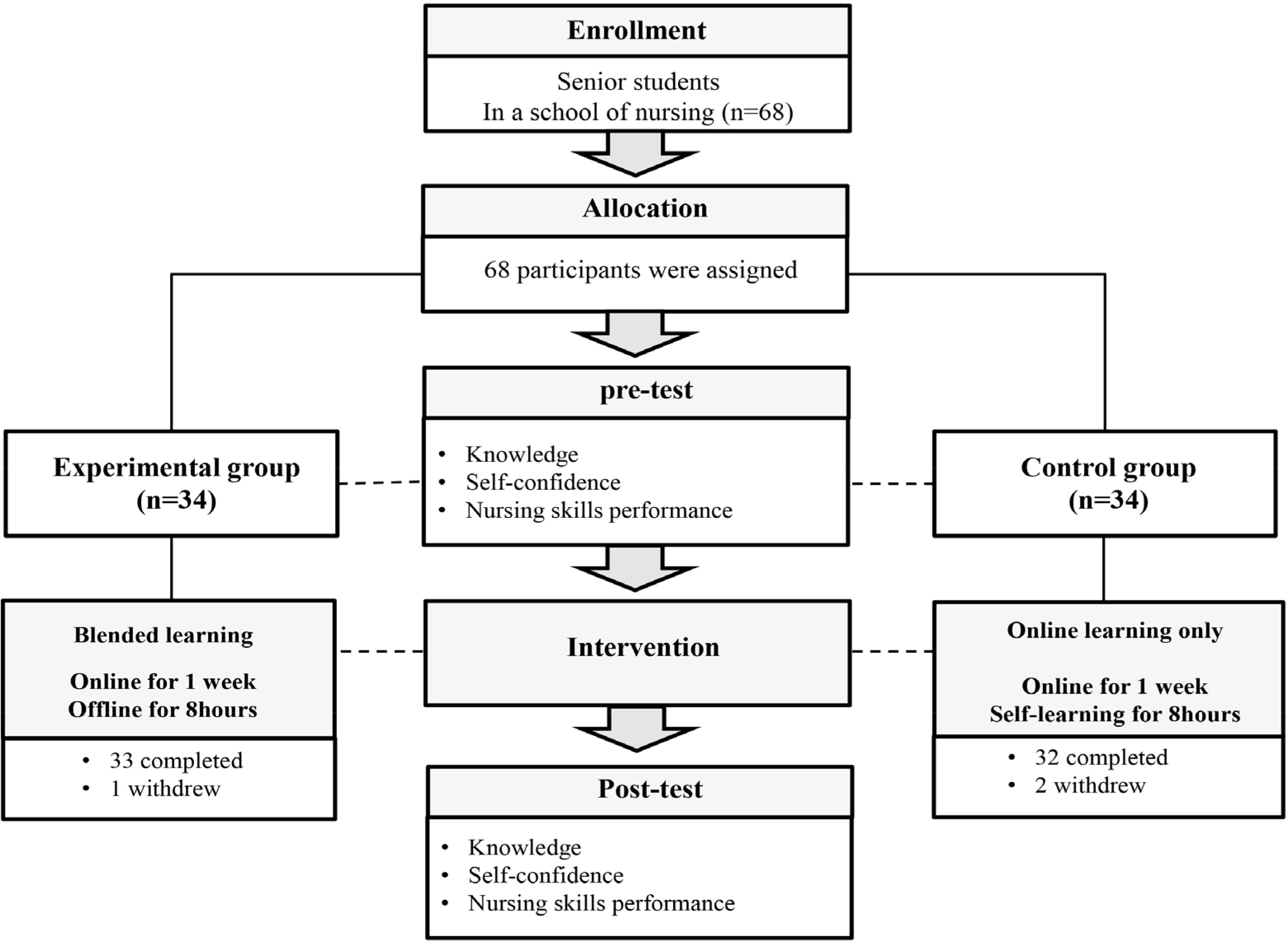
Subjects were students who took a course in the “ adult healthy nursing” curriculum, including theory about res-piratory disease and mechanical ventilation, at a college located in Incheon. Students in their 4rd year who were scheduled to practice in an intensive care unit (ICU) were recruited. The effect size was set to .70 based on mean dif-ference between groups divided by standard deviation from result of a previous study [17]. Using G∗power pro-gram 3.1.9 and with a power (1-β) of .80, a significance lev-el of .05, and an effect size of .70, two-tailed independent t-test resulted in a sample size of 34 people per group. Convenience sampling was performed by the researcher in each of 4 practice groups of less than 20 people. Initially, 70 people participated. However, five subjects did not respond to the follow-up. The reasons for dropping out were all personal circumstances, such as job interviews. There-fore, 33 subjects in the experimental group with blended learning and 32 subjects in the control group with online education only were included in the final analysis (Figure 1).
3. Development Procedure
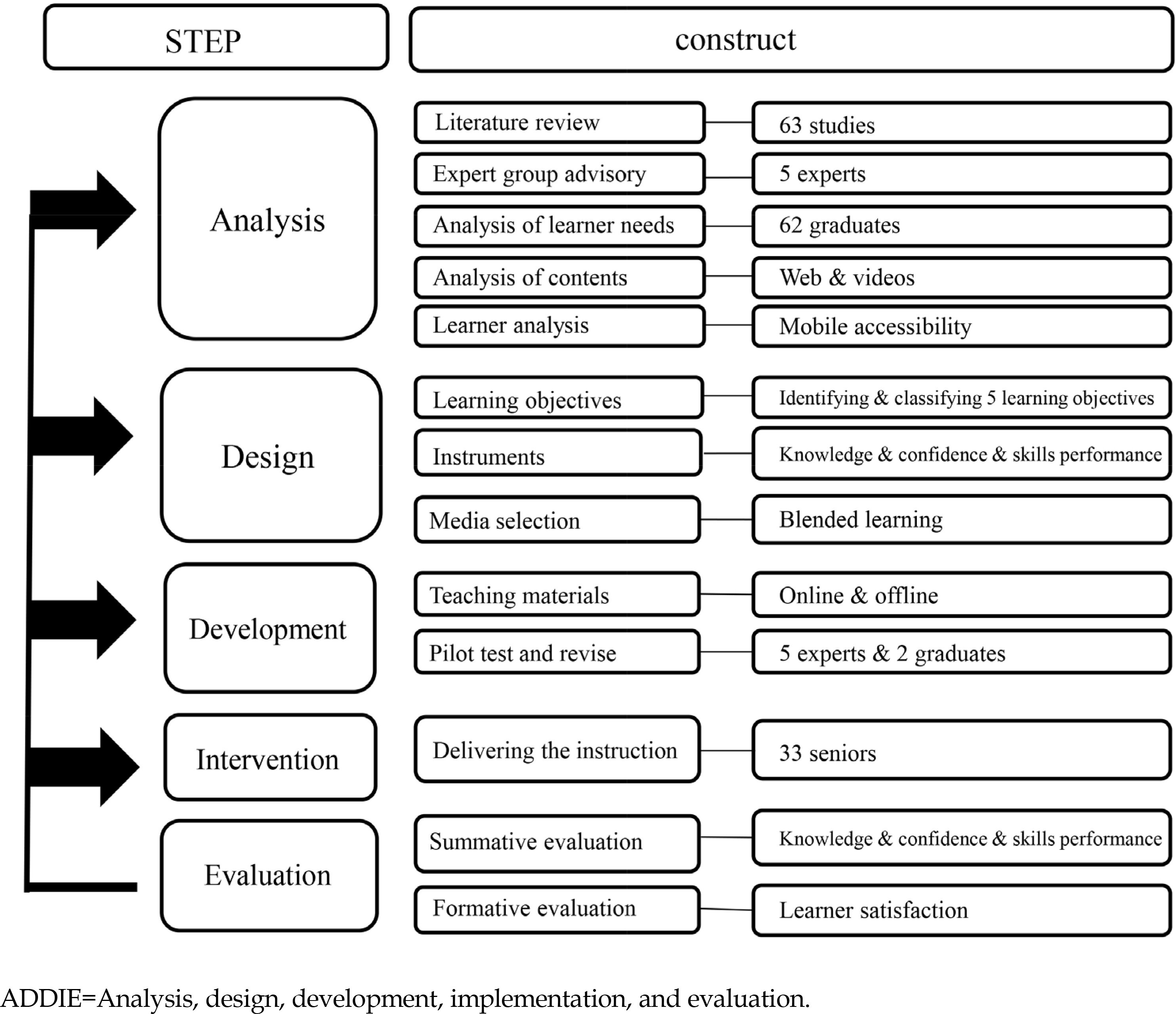
This program was developed based on the analysis, design, development, implementation, and evaluation (ADDIE) model (Figure 2). This is a procedural model used for instructional systems design (ISD) and is the most basic model used to achieve an efficient and attractive teaching system based on learner's needs [18].
1) Analysis
Literature review. After searching for “ ventilator” or “ blended learning” in domestic and international academ-ic search engines (KISS, DBpia, CINAHL, MEDLINE), 34 domestic and 29 foreign studies were reviewed to analyze the contents and methods of education, educational de-mand, and influencing factors. As a result of a literature review, there were educational research on ventilator-re-lated infection management [5–7], web-based ventilator education program [8–10], and simulation education program [11–13]. Also, it was confirmed that blended learning is a teaching method that can efficiently utilize learning time and increase learner satisfaction. Therefore, it was de-cided to apply blended learning as a teaching method to improve ventilator-related knowledge and skills.
Expert group advisory. The researchers asked for ad-vice from a group of experts. Three adult nursing pro-fessors and two advance practice nurses (APNs) in critical care nurse team, provided advice on the content and direction of the mechanical ventilation education program. After the contents of the advisory were reviewed, it was suggested that ventilator education is an essential topic for nursing students and is a core skill that is essential in the field. In addition, the researchers and experts agreed that conducting the education program at a time when various mechanical ventilators had recently been developed and used was timely. Experts said that it was necessary to ap-ply and construct a teaching method that allows students to fully understand basic concepts and terms and learn repeatedly. After analyzing the existing website and vid-eos related to ventilator education to determine the pro-gram's primary content, a secondary expert consultation was requested to insert and modify additional contents, select measurement tools, and distribute offline and on-line contents.
Analysis of learner needs. In order to compose the edu-cation content, difficulty, and method desired by the lear-ner, the learner needs were first investigated. In February 2020, a survey was conducted with 62 graduates who had already completed the fourth-year curriculum. The survey items addressed the necessity, contents, and method of ventilator training. The analysis results showed that 90.3% of the respondents recognized that ventilator training was necessary. For particularly difficult parts, such as under-standing ABGA and applying ventilator nursing skills, they wanted an educational composition including videos and hands-on practice.
Analysis of existing website and videos. Prior to the de-sign of the LMS for online learning and the production of videos, the previously produced videos and websites were analyzed. The educational website operated by the do-mestic nursing college was mainly to provide knowledge, and the YouTube videos produced by the institution were the level of explaining the operation method for medical personnel. They were collected for analysis of educational topics, content development methods, and planning intentions. Since it was confirmed that all students owned smart-phones, it was possible to post study materials through LMS, check student attendance, and check assignments.
2) Design
Learning objectives. Based on the results of the analysis phase, five objectives for mechanical ventilation education were set for college students, and a total of 14 subgoals to be performed were also set (Table 1).
Table 1.
Structure of the Education Program with Blended Learning for Nursing Students
Assessment instruments. To evaluate whether the learn-er had reached 5 objectives, instruments developed by this researcher.
Media selection. It was selected as a blended learning teaching method that combines online and offline learning.
3) Development
Development and production of teaching materials.
• Text & videos: Text data on respiratory physiology and ventilator management were loaded into the LMS of the researcher's university. It summarizes a large number of learning ranges and helps to repeat learning. Two lecture videos created by this researcher (ABGA, ventilator terminology) and one video dem-onstration by the researcher (ventilator nursing skills) were loaded into the LMS.
• Quiz & Q&A: Learners can repeat the quiz at any time by accessing LMS. This helps with learning difficult concepts or terms. In the online Q&A section, the re-searcher answered any questions that learners asked.
• Mechanical ventilator & operation manual: A port-able ventilator (model: MTV 1000) provided at the university to which this researcher belongs was used.
• Simulator: To serve as a patient to connect with the ventilator, SimMan 3G of Laerdal™ products in the nursing lab of the university to which this researcher belongs was utilized.
• ABGA result sheet & hand-over notes: The person in charge of the next shift was given the details of the patient during hand-over, including the patient's con-dition and test results.
Pilot test and revise. After two graduates reviewed the material primarily using the developed online texts and videos, we received feedback on the degree of under-standing and difficulty, typos, terms, and images. The contents of the program were finalized after deliberation among the researcher, three nursing professors, and two APNs.
4) Intervention
The experimental group was provided with 1 week of online learning and 8 hours of offline learning from July 13, 2020 to July 23, 2020 and the control group was pro-vided with 1 week of online learning and 8 hours of self- learning from July 6, 2020 to July 16, 2020. In order to mini-mize contamination between groups, the intervention was applied to the experimental group after 1 week.
First, to achieve the learning objectives, online learning is developed in the form of text, videos, quiz, Q&A, oper-ation manual, and performance checklist and then up-loaded to LMS. The researcher notified both groups to do online learning for a week and guided them to the learning method. Researcher encouraged students to complete their learning 2 hours a day while checking their learning status. So all the students studied at least 10 hours in a week.
After a week of online learning, researchers provided an offline learning (hand-over, simulation, and peer learning) and follow-up activities (analysis of test results, man-ual learning, operation, and writing a reflection on one’ s feelings) to the experimental group in a practice room of the college for 8 hours. The simulation was conducted so that the students practiced the procedure repeatedly. Peer learning was shared with peer students to perform prac-tice and handover. The two practice groups of less than 20 people who were sampled in the experimental group, each received offline learning on different days.
After a week of online learning, the control group per-formed an self-learning under the supervision of a practical assistant in a practice room of the college for 8 hours. During self-learning, online learning was repeated and follow-up activities were performed individually. Also the two practice groups of less than 20 people who were sampled in the control group, each received self-learning on different days. The composition and contents of the program are presented in Table 1.
5) Evaluation
To evaluate the learner satisfaction, 65 subjects were surveyed for learner satisfaction with four questions imme-diately after the end of the intervention period. The satis-faction of the experimental group had an average score of 4.64±0.78 points (out of 5 points), and that of the control group had an average score of 4.34±0.79 points (t=1.50, p=.138). The satisfaction of the experimental group with the amount and time of learning had 4.52±0.80 points, and that of the control group had 3.91±0.93 points (t=2.84, p= .006). The satisfaction of the experimental group with the composition and difficulty level of contents had 4.73±0.45 points, and that of the control group had 3.97±0.74 points (t=5.00, p<.001). The most interesting parts of the experi-mental group were applying ventilator nursing skills in hands-on practice (46.2%) and the video related to venti-lator nursing skills (23.1%).
4. Measures
1) Knowledge of ventilator
Knowledge of mechanical ventilation instruments is ad-dressed by multiple-choice questions developed by a re-searcher in the course of the development of this educational program. Based on the sub-goals of the program, the item-content validity index (I-CVI) of 5 experts (3 adult nursing professors and 2 APNs) is calculated. The final 20 questions were selected because, after being tested for con-tent validity again, they had a value of .80 or higher. The subarea of the instrument consisted of respiratory physiol-ogy, ABGA, ventilator terminology, and ventilator man-agement. This instrument gives 1 point for a correct an-swer and 0 points for an incorrect or unknown answer. The scale ranges are 0 points for the minimum value and 20 points for the maximum value. The higher the score is, the higher the degree of the subject’ s knowledge related to mechanical ventilation is. The internal reliability, Kuder- Richardson 20, of this scale was .84.
2) Self-confidence
The ventilator nursing practice self-confidence instru-ment was developed by a researcher during the course of this educational program’ s development. Based on the sub-goals of the program, 5 experts’ I-CVIs were calcu-lated, and the final 10 questions were adopted. The ven-tilator nursing practice confidence instrument is a 10-point scale consisting of explanation, assessment, and intervention. The minimum value is 0 points, and the maximum value is 100 points. The higher the score is, the higher the subject’ s self-confidence is. The internal reliability or Cron-bach’ s ⍺ of this scale was .96.
3) Ventilator nursing skills performance
The ventilator nursing skills performance instrument is a checklist developed by a researcher during the course of developing this educational program. Based on the sub- goals of the program, the I-CVIs of 5 experts are calcul-ated. The final 20 questions were consisted of preparation, intervention, and evaluation. Each question was rated on a 2-point scale, with 0 points for “ not performed,” 1 point for “ partially performed,” and 2 points for “ performed enough.” The scale ranged from 0 to 40, and the higher the score is, the higher the subject’ s performance ability is. Two evaluators measured each and calculated an average value. Intra-class correlation (ICC), comparing the meas-urements of the two raters, was 0.94, and the internal reli-ability Cronbach’ s ⍺ of the scale was .90.
5. Data Collection
The period of data collection was from May 16, 2020, to June 30, 2020. This study was conducted with the approval of the Institutional Review Board of the university in Seoul to protect the ethical concerns of study subjects (2-7001793 −AB-N-012020001HR). All the recruiters were provided with online format explanations describing voluntary par-ticipation, guarantee of anonymity, possibility of with-drawal, disadvantages, and harmlessness. The researcher obtained online informed consent from the subjects before they participated in the study. It was explained that all in-terventions and investigations are for research purposes and would not affect subjects’ grade evaluations. The co-researchers conducted the intervention directly. Data collection and intervention providers were conducted by different researchers.
After the follow-up investigation, the control group was provided the same offline learning program. Preliminary investigations were conducted on the same day for each group, and follow-up investigations were conducted im-mediately after the intervention. Both pre- and post-inves-tigation were conducted with online questionnaires, ex-cept for the ventilator nursing skills performance. To measure the subjects’ ventilator nursing skills performance, two raters scored each checklist. Researcher involved in the data analysis and two raters didn’ t know which group was offered intervention.
6. Data Analysis
Collected data were analyzed using the jamovi 1.1.9 version program. The dependent variables and the gen-eral characteristics of the subjects were analyzed using de-scriptive statistics. It was analyzed with an independent t-test to verify the hypothesis and prior homogeneity of the experimental and control groups.
RESULTS
1. Homogeneities between the Experimental Group and the Control Group
Regarding the general characteristics of study subjects, there were 15 males and 50 females. The average age of the subjects was 24.75±4.70 years old (t=−0.57, p=.570). As a result of confirming the adult nursing grade score before the study, homogeneity was secured between the two groups (t=−0.65, p=.521). As a result of comparing prior knowledge of mechanical ventilation (t=0.70, p=.485), pri-or self-confidence (t=−0.52, p=.606), and prior ventilator nursing skills performance (t=−1.34, p=.184) between the two groups, there was no significant difference in total scores. These results are summarized in Table 2.
Table 2.
Homogeneity Test between Experimental and Control Groups (N=65)
2. Testing of Hypotheses
As a result of analyzing the collected data to test hy-pothesis 1, the control group's knowledge difference be-tween their pre- and postscores was 6.69±4.29, and the experimental group's knowledge of mechanical ventilation difference between their pre- and postscores was 10.85 ±3.50. As a result of testing differences between the two groups, the average score of the experimental group was significantly higher than that of the control group (t=4.29, p<.001). Among the knowledge questions, subjects’ scores on characteristics of ABGA (t=2.79, p=.007), characteristics of ventilator terminology (t=4.64, p<.001), and ventilator management (t=3.80, p<.001) were significantly higher in the experimental group, but scores were not higher for the characteristics of respiratory physiology (t=−0.85, p=.399) (Table 3). Thus, hypothesis 1 was supported.
Table 3.
Comparison of Knowledge, Self-Confidence, and Ventilator Nursing Skills Performance between Experimental and Control Groups (N=65)
As a result of analyzing the collected data to test hy-pothesis 2, the self-confidence difference between the preand postscores of the control group was 61.53±18.38, and that of the experimental group was 72.42±19.64. As a re-sult of testing differences between the two groups, the average value of the experimental group was significantly higher than that of the control group (t=2.31, p =.024). Among the self-confidence questions, explanation (t=2.21, p=.031), assessment (t=2.16, p=.034), and intervention (t= 2.21, p=.031) were significantly higher in the experimental group (Table 3). Thus, hypothesis 2 was supported.
As a result of analyzing the collected data to test hy-pothesis 3, the ventilator nursing skills performance dif-ference between the pre- and postscores of the control group was 14.86±10.71, and that of the experimental group was 26.03±8.57. As a result of testing differences between the two groups, the average value of the experimental group was significantly higher than that of the control group (t=4.65, p<.001). Among the ventilator nursing skills per-formance questions, preparations (t=4.35 p<.001), inter-vention (t=3.49, p=.001), and evaluation (t=4.44, p<.001) were significantly higher in the experimental group (Table 3). Thus, hypothesis 3 was supported.
DISCUSSION
This program was developed according to the ADDIE model and was developed cyclically through the process of feedback conducted at each phase. An important factor in the analysis phase for educational program develop-ment was learner-analysis activities. This study has gone through literature review and surveys. In addition, the reliability of the program was increased by receiving expert advice twice during the analysis stage.
In the design stage, it was decided to apply blended learning, which was thoroughly reviewed during the anal-ysis process. In this study, offline and online contents were appropriately distributed by applying blended learning, a teaching method that can efficiently use class time and in-crease student interest [14]. And the skills that require re-petitive training were demonstrated by peers and prac-ticed repeatedly so that learners' autonomy could be maxi-mized [19,20]. In terms of the proportion of blended learning, this program consisted of 40% skills-oriented offline and 60% knowledge-oriented online learning.
In the development and intervention stage, text materi-als and videos were mounted on the LMS, and after online learning, it was done through flip learning, in which learn-ers participated in offline classes [21,22]. Due to COVID 19 pandemic, we measured the instruments with an online questionnaire. Since the practice was originally a small study of less than 20 people, there were no difficulties in progressing according to the planned intervention. It was rather easy to apply blended learning to students who had already experienced online learning.
In the evaluation stage, the experimental group to which blended learning was applied exhibited a higher degree of knowledge after the program than the control group, with which only online learning was used, and the difference in confidence and ventilator nursing performance was sig-nificantly higher in the experimental group. In a previous study comparing clinical supervisor skills after applying blended learning and online learning to nursing students, the group’ s knowledge and satisfaction with blended learning was significantly higher than that of online learning [23]. And a research of blended-learning approach to public health services training resulted in a higher know-ledge achievement and satisfaction level compared with a pure e-learning [24]. In addition, many studies comparing blended learning with traditional education have shown that blended learning has a positive effect on knowledge or skills of the various learning contents [25–28].
In this study, it was found that the overall satisfaction level of learning was similar for both groups. But the ex-perimental group, which applied blended learning, was more satisfied with the amount of learning, time spent, composition and difficulty level of contents. In particular, the most interesting sections were the hands-on practice and demonstration videos related to ventilator nursing skills. The common theme of the impressions that students wrote after blended learning was that they became con-fident in the skills they recognized as difficult. Doing a practice activity was an educational method that achieve the most similar effect to the actual situation by performing personally, and video was a lively and excellent trans-mission of effective material [29]. The educational pro-gram composed by mixing them had three conditions of experiential learning: intention, structure, and context [30]. It is considered that repeat watching the instructor’ s dem-onstration videos before performing the hands-on practice can make a difference, showing that the blended learning was effectively utilized. Therefore, Blended learning pro-vided added pedagogical value when compared to online learning in terms of teaching students ventilator nursing skills. The cons of blended learning is that designing two or more teaching methods absolutely requires the effort of an instructor. However, as it is a learning method that in-creases student interest and satisfaction, it should be ap-plied widely in the future.
The limitation of this study was that it was conducted with students from a single college. Therefore, caution is needed when generalizing results of this study. In addition, since it was measured with a non-standardized scale, it is necessary to develop and apply instruments with high validity in the future. Despite the limitation, the importance of the practice-related skills has been emphasized in the nursing curriculum recently, so we propose that the program of this study can be used not only for education and study for clinical practice but also for simulation prac-tice and core nursing skills. Furthermore, blended learning can be applied to nursing students as well as medical personnel, and there is a possibility to improve quality of care and patient safety.
CONCLUSION
This study developed a mechanical ventilation education program with a blended learning method for nursing students and verified its effectiveness. For the develop-ment of this program, a learner-centered ISD process was applied by thoroughly analyzing learners’ educational needs, and feedback was obtained for each phase. As a re-sult of the verification of this program, the experimental group participants improved their knowledge, self-con-fidence, and nursing skills performance level compared to the control group. Therefore, all effects were proven as hypothesized. This program contributed to enhancing nursing performance ability by including learners’ actual practical activities and online learning. It is meaningful that knowledge and skills that students consider difficult and complex to obtain can be sufficiently learned through well-organized teaching methods such as blended learning.
Regarding suggestions for the use of this program and subsequent research, first, longitudinal studies are needed in the future to confirm the long-term effects of educational programs. Second, it is necessary to conduct a pro-gram-effectiveness verification for nursing students lo-cated in various regions. Third, it is necessary to minimize the possibility of bias and error by conducting a random-ized controlled trial.


